40 year old lady presented with progressive weakness of all four limbs of 2 weeks duration. On evaluation in the out-patient clinic, she was walking with support with grade 4/5 power and spasticity in all four limbs.
Her MRI scan was suggestive of cord compression at C7-D1 level. The lesion appeared to be primarily bony causing destruction of the right half of the vertebral body with intra-spinal extension and cord compression. CT scan revealed erosion of the C7 vertebral body with bony cortex intact.
Possibility of “Aneurysmal Bone Cyst” was considered. In view of deficits, she underwent anterior approach, C7 vorpectomy, and fusion with titanium cage and plates and screws was done. Intra-operatively, the tumor was fleshy bluish red, causing significant cord compression. Following corpectomy, dural sac became lax and pulsatile. In view of associated dorsal compression, second stage posterior decompression (C7-D1 laminectomy) was done in the same sitting.
Patient tolerated the procedure well and recovered neurologically. Her post op X-ray showed implant in position.
3 month follow up MRI showed no residual contrast enhancing lesion with decompressed cord. She has recovered neurologically and is walking independantly with no neurological deficits.
Aids used: 3D-Carm, Neurosurgical drill

Figure 1a: T2W Sagittal showing tumor with significant cord compression

Figure 1b: Coronal T2W image with extradural tumor on left causing cord compression

Figure 1c: T1W with contrast with significant cord compression
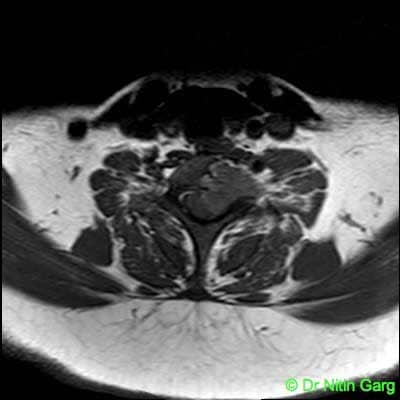
Figure 1d: Axial contrast MRI showing left sided body tumor with extension into the canal and cord compression

Figure 2a: 3 months follow up MRI with no residual tumor and decompressed spinal cord

Figure 2b: Follow up T2W MRI with decompressed spinal cord

Figure 2c: Follow up Axial MRI with no cord compression

Figure 2d: Follow up X-ray with implant in-situ






