Spinal fractures are associated with significant morbidity and loss of work. There is a subgroup of fractures wherein patients have significant bony injury but no neurological deficits. Traditionally, such patients were managed with bed rest for upto 3 months. Prolonged bed rest itself is associated with morbidity and loss of income. Minimally invasive methods of fixation are very useful in such patients as it allows for spinal fixation using smaller incisions, faster recovery and faster return to their occupation.
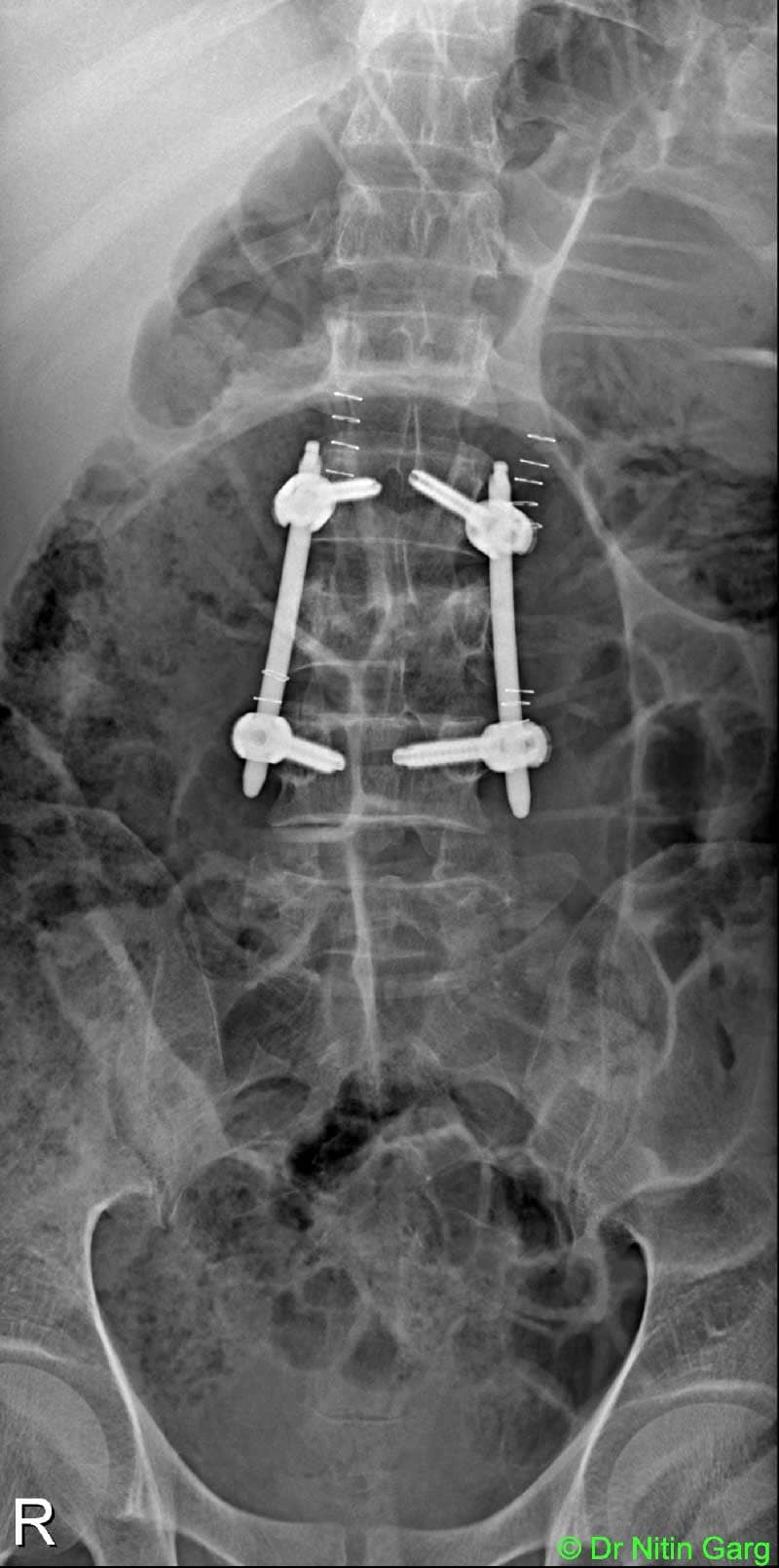
A 45 year old patient wad admitted with h/o fall from height. There was no neurological symptoms apart from back pain. Imaging was suggestive of a stable burst fracture with no significant retropulsion of the bone fragments. Option of conservative management with bed rest and Percutaneous transpedicular screw fixation was given. Patient underwent minimally invasive Percutaneous Transpedicular screws fixation incorporating adjacent levels on either sides. He was mobilised on the second day and was discharged on 4th post-operative day. By 2 weeks, he was back in his office.
Aids used: Percutaneous transpedicular screw system, 3D C-arm.
“Percutaneous Transpedicular Screw system” is a newer and minimally invasive method of inserting transpedicular screws into the lumbar and lower dorsal spine. In this method, the pedicles are cannulated using PAK (Percutaneous access kit) needles under C-arm guidance. Long Steinman wires are passed, PAK needles removed and cannulated screws inserted by rail-roading over the Steinmann wires. Separate stab incisions are given for each screw (about 2cm length) and the rods is tunnelled in subfascial plane using various methods – arc based or free hand method.
3D C-arm provides for the axial image after the wires are cannulated. It allows for on-table confirmation of the exact location of the wire and detects on-table breach of the pedicle so that correctionas can me made immediately.
a