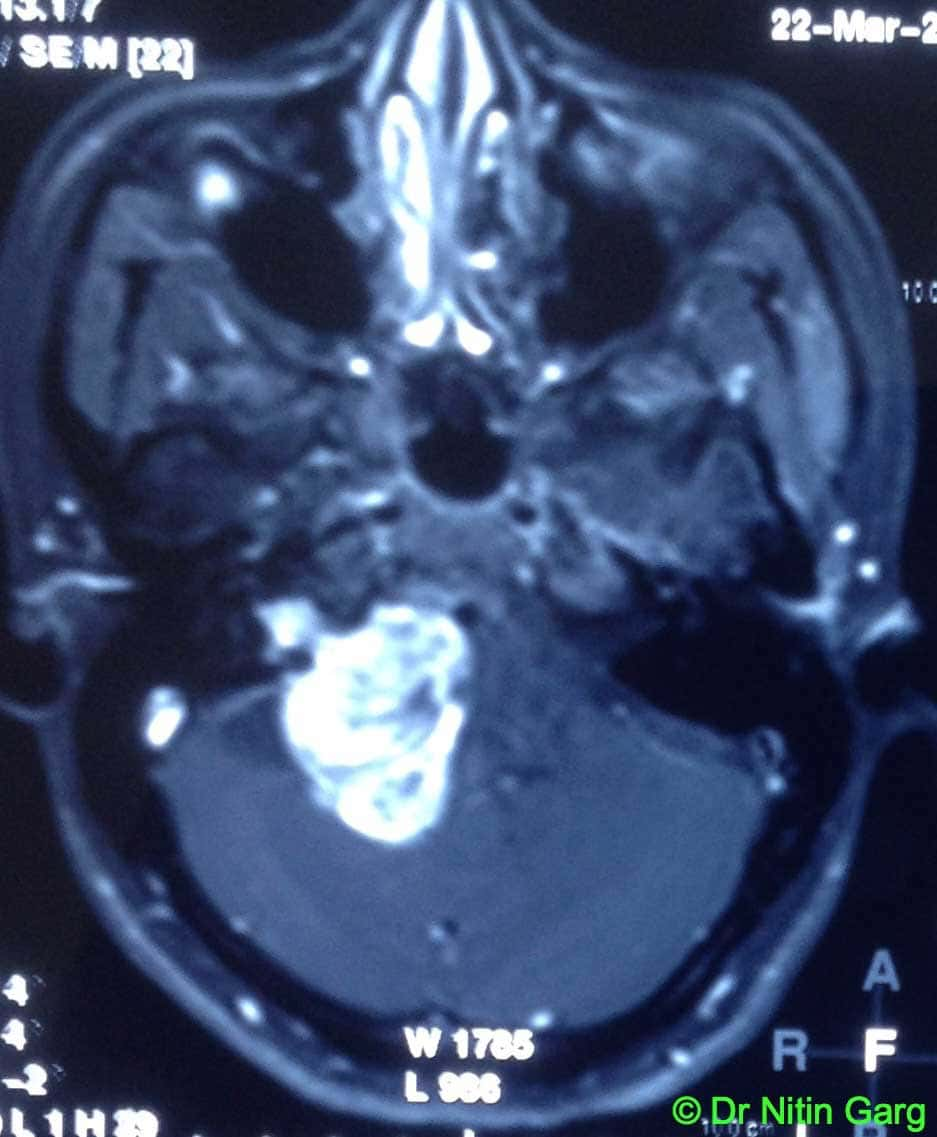
45 year old lady presented with right sided hearing loss and gait ataxia. Her imaging was suggestive of a right sided tumor in the cerebello-pontine angle with contrast enhancement and extension into the internal auditory meatus s/o Acoustic Schwanomma.
Right retromastoid suboccipital craniotomy and near total excision of the tumor was done using microscopic neurosurgery methods. Additional intra-operative aids used were “Intra-operative Neurophysiological Monitoring (IOM) ” and “Ultrasonic Aspirator (CUSA)”.
Setting up of IOM requires needle electordes to be inserted into the orbicularis oculi, orbicularis oris (for Facial nerve monitoring) and into the masseter (for Trigeminal Nerve monitoring). Anaesthetists are informed In advance about the need for IOM so that muscle relaxants are avoided when the monitoring is being done. Impulses are obtained if the stimulating probe / surgical dissection site is in close proximity to the facial and trigeminal nerve. By using this aid, the incidence of injury to the facial nerve is reduced significantly and tumor can be removed safely.
CUSA helps in faster removal of the tumor with lesser incidence of injury to the facial nerve.
Intra-operatively, the facial nerve was encountered towards the end and the capsule could be dissected off with anatomical and electrophysiological preservation of the facial nerve. Internal auditory meatus was drilled and intra-meatal portion of the tumor was also removed. A thin layer adherent to the nerve near the meatus was left behind (Follow up scan)
Aids used: microscope, neurosurgical drill, CUSA, neurophysiological monitoring