Case-1
Tumors located adjacent to the eloquent cortex / regions have a high chance of neurological deficit if operated conventionally under anaesthesia. Awake craniotomy in these patients allows for safe excision of the tumor with minimal morbidity.
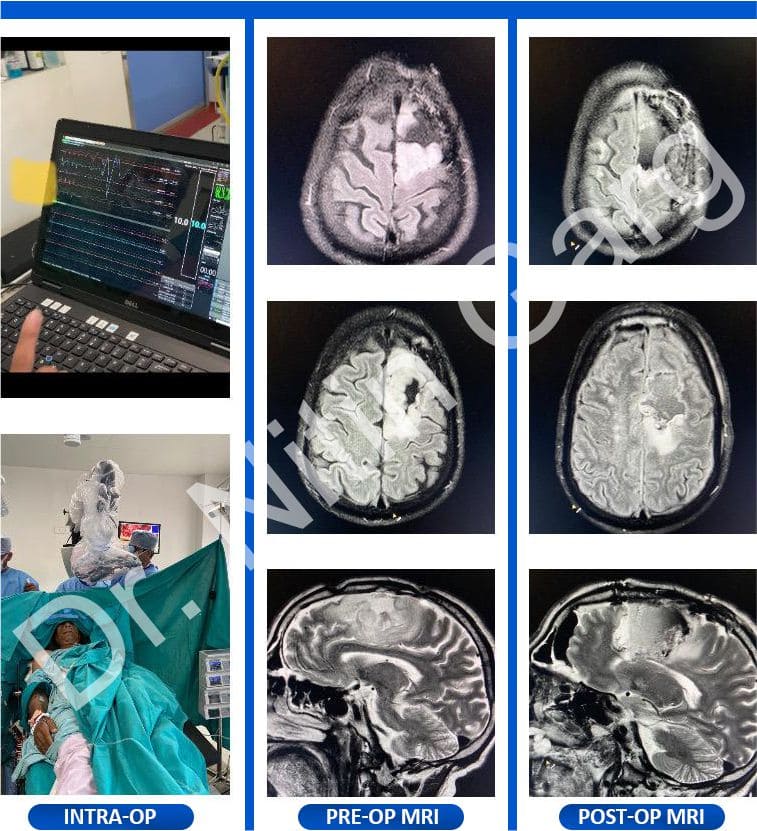
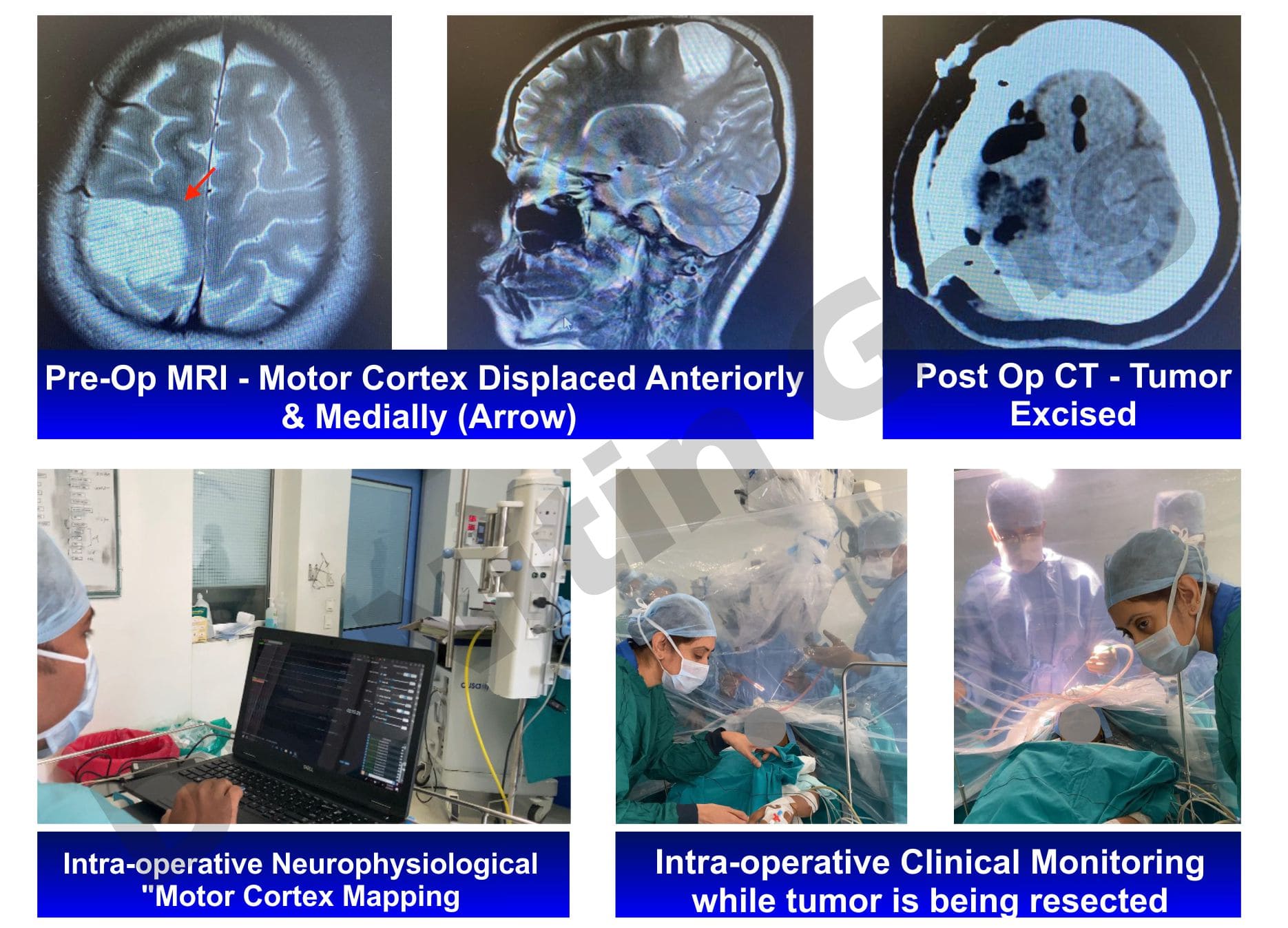
In the first column, the patient had tumor in posterior frontal lobe with involvement of motor cortex. She underwent awake craniotomy and safe removal of the tumor without any deficits by continuously monitoring the movements of the contralateral limbs. The posterior limit could be reached safely upto the motor cortex (as seen in post-op image)
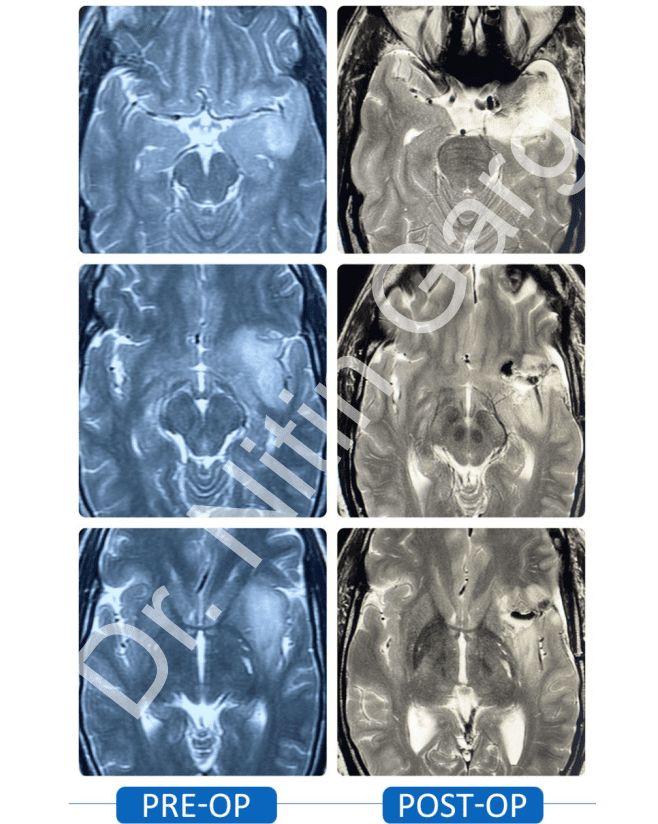
In the second column, the patient had a tumor in left posterior temporal lobe, in close proximity to the speech area. He too underwent awake craniotomy with continuous monitoring of speech while removing the tumor. Post-op scan shows adequate removal of the tumor with no deficits in speech.
Aids used: Neuro-navigation, microscope, CUSA.

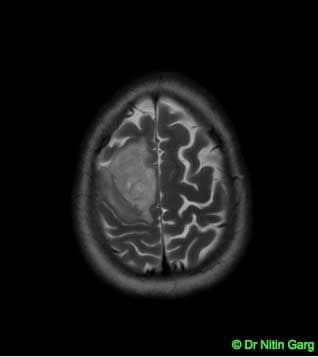 Pre-op MRI with tumors abutting and involving the motor cortex
Pre-op MRI with tumors abutting and involving the motor cortex
.jpg) Post-op MRI shows tumor excised upto the motor cortex with intact motor cortex.
Post-op MRI shows tumor excised upto the motor cortex with intact motor cortex.
.jpg) Left temporal heterogenously enhancing mass lesion
Left temporal heterogenously enhancing mass lesion
.jpg) Post-op CT with adequate removal of the tumor
Post-op CT with adequate removal of the tumor